VERIFICATION OF ENDOTRACHEAL TUBE PLACEMENT: A BRIEF SYNOPSIS
D. John Doyle MD PhD
April 2004
djdoyle@hotmail.com
Scope of the Problem
In one study of cardiac arrests “due to anesthesia”, four of 27 were due to unrecognized esophageal intubation. In a review of anesthetic malpractice claims, seven of 192 complications resulting in cardiac arrest, brain damage of death were from esophageal intubation. A British study of anesthetic accidents from 1970 to 1977 revealed 50 cases of accidental esophageal intubation resulting in death or brain damage. A similar review listed esophageal intubation as the main anesthesia related cause of death or neurologic damage. An Australian study of anesthesia mortality rate showed 69% of deaths to be airway related, many of these being esophageal intubations.
Even more common is unrecognized bronchial intubation. One study showed six of 38 ER intubations were right main stem intubations detected only on CXR. Another study showed a 28% incidence of right main stem intubation by ACLS certified physicians. A 9.6% incidence of right main stem intubation was noted in a prospective study of 354 ICU patients. Bronchial intubation is associated with atelectasis, tension pneumothorax and hypoxia in many cases.
Detecting Esophageal Intubation
1.  Direct Visualization of ETT Going Through Cords
Direct Visualization of ETT Going Through Cords
Gold standard, but not always achievable. Also, the ETT may be unintentionally withdrawn while securing the tube or with positioning of the patient. Furthermore, extension or lateral rotation of the neck can cause cephalad movement of the tube, resulting in extubation.
2. Chest Movement
In the patient with large breasts, obesity, barrel chest, etc. chest movement may be difficult to evaluate. Also, chest movement simulating lung ventilation can be seen with esophageally positioned tubes (cadaver studies). Unreliable method.
3. Breath Sounds
The literature documents numerous cases where apparently normal and symmetric breath sounds were present with esophageal intubation.
4. Epigastric Auscultation
Some clinicians auscultate to ensure absence of air entering the stomach. But vesicular breath sounds can be transmitted to the epigastric area in thin tracheally intubated patients. Observing the belly for gastric distention ay be unreliable with hiatal hernia or intrathoracic GI contents (eg. gastric pull-up), while observed gastric distention might be due to mask ventilation prior to intubation.
5. Presence of Exhaled Tidal Volumes
Tidal volumes up to 180 ml and peak flows up over 50 L/min may occur with the esophagus intubated and the trachea obstructed while spontaneous respiratory efforts are being attempted. Thus, reservoir bag movement may appear to be satisfactory under such circumstances.
6. Reservoir Bag Compliance
The impression of abnormal reservoir bag compliance may lead one to suspect an esophageal intubation. However, compliance may vary widely from person to person and repeated filling and emptying of the stomach leading to inflation and deflation of the breathing bag can be mistaken for pulmonary ventilation.
7. Tracheal Tube Cuff Maneuvers
With the cuff deflated, the higher pitched sound of air escaping around a tracheal tube, compared to the more gutteral sound of leakage around an esophageal tube, has been used as a distinguishing feature but is not particularly reliable. Palpation of the tracheal tube cuff in the neck to verify position has been reported to fail, perhaps because the distensible esophagus simply balloon outwards. The cuff volume needed to stop a leak can also be a sign of incorrect tube position; excessive cuff volume can be an indicator of esophageal intubation. Also, excessive cuff volumes may be required with the cuff at or just above the level of the cords.
8. Tube Condensation
The presence of condensed water vapor in the tube lumen is not guarantee of tracheal intubation. Not helpful.
9. Chest Radiography
Roentgenographic recognition of esophageal intubation can be difficult without a lateral view unless the tip is seen below the carina or gastric dilation is present. Not practical.
10. Fiberoptic Bronchoscopy
Visualization of the tracheal rings and carina with the fiberoptic bronchoscope (FOB) through the ETT is a reliable method (but the method is relatively expensive and the FOB is prone to breakage).
11. Tracheal Palpation
Palpation of the trachea in the sternal notch during intubation by another person can be used to help verify tube position. An old washboard-like sensation can be appreciated as the tube passes over the tracheal rings. This sensation is not present if the tube is in the soft posterior lying esophagus.
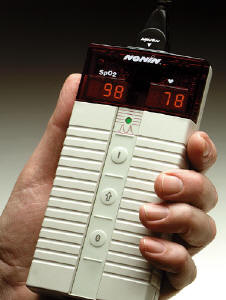
12. Pulse Oximetry
Desaturation may be a late sign of esophageal intubation, especially with preoxygenation.
13. Capnography
Most reliable method for routine clinical use. Although CO2 can sometimes be detected initially with esophageal intubation, the end-tidal CO2 is low in such cases, the wave pattern is irregular and the CO2 levels rapidly diminish with repeated ventilation. However, with severe bronchospasm or with cardiac arrest, capnography may not detect a correctly placed tube.
14. Easy Cap®
This is a colorimetric method that can be used to detect expired CO2. Just attach the detector to the endotracheal tube and begin monitoring CO2 breath by breath. A color change between inspiration and expiration helps you verify proper ETT placement in seconds. It also helps you to monitor ETCO2 during CPR. The color changes from purple to to yellow when CO2 is expired.
15. Ambu Tubechek®
The Ambu Tubechek is a device that easily confirms if endotracheal tube placement is correct or not. It is based on anatomical differences between the esophagus and trachea. Simply empty the device of air (by squeezing) and attach to the ETT. If you can aspirate air, you are in the trachea. If the tube is in the soft, unsupported esophagus, the esophageal walls will collapse around the end of the endotracheal tube when you attempt to aspirate air. This method has an important advantage over capnography in that it works even when there is no cardiac output. And since no initial ventilation is needed, the potential for stomach inflation is reduced.
Detecting Bronchial Intubation
Right main stem intubation is quite likely to occlude the origin of the right upper lobe, given the proximity of that lobe’s takeoff to the tracheal bifurcation. RUL collapse may cause substantial V/Q mis-matching, but may exist without classic signs such as cyanosis, tachycardia, tachypnea or hypotension. Left main stem intubation is less common but does occur. Factors contributing to the more frequent occurrence of right bronchial intubation are its greater width and less acute angle of departure from the trachea. Also, the right-sided bevel of the standard ETT tends to guide the tube preferentially down the right side. Simple flexion of the intubated patient’s neck can result in bronchial intubation. In one study, the ETT moved an average of 1.9 cm away with extension. Movements up to 5 cm were noted in some cases.
1. Breath Sounds
Chest auscultation with bronchial intubation be equivocal. In one study, ETT’s were advanced into the right main bronchus in 49 adults, then withdrawn until the breath sounds were equal. CXR’s were then taken. The tube tip remained in the right main stem bronchus in 25 of these patients despite equal breath sounds.
2. Tracheal Tube Cuff Maneuvers
Injection of sterile saline into the pilot cuff, followed by gentle compression of the pilot cuff while auscultating over the suprasternal notch, is another way of checking proper position. The characteristic gurgling sound is not heard if the tip is in a main stem bronchus or near the carina.
3. Chest Radiography
The tube tip and carina can be located on CXR. When the carina is not visible, it is opposite T6 +/- 1 vertebrae (T5 to T7). In adults, the cords are at C5/6. In the neutral position, a safe tip level is T2 to T4. In adults, the distance between tube tip and carina should be 3.5 cm with the neck flexed, and 7 cm with the neck in the neutral position. In infants, the tip should be at least 2 cm above the carina and 1.5 cm below the cord in the neutral neck position.
4. Tube Position Calculations
Aim for 21 cm at lips in normal-sized females and 23 cm in normal-sized males. In children, the airway length (incisor teeth to mid trachea) is given by height (cm)/10 + 5 cm. Also the 7-8-9 rule can help: infants weighing 1 kg: 7 cm at lips; 2 kg: 8 cm; 3 kg: 9 cm. For nasal intubation in children, the tube length should be height (cm) x 0.16 + 4.5 cm. Leave 2 cm of tube outside the nostril in infants and 3 cm in older children. Also, pediatric tubes have a black safety line designed to be placed at the level of the vocal cords.
5. Fiberoptic Bronchoscopy
Troublesome but accurate.
Sources
1. Birmingham PK, Cheney FW. Incorrect tube placement. Prevention of a fatal complication. Problems in Anesthesia 1988; 2: 278-291.
2. Birmingham PK, et al. Esophageal intubation: A review of detection techniques. Anesth Analg 1986; 65: 886-891
3. Roy RC. Esophageal intubation. Anesth Analg 1987; 6: 482
Abbreviations
CXR chest x-ray
ER emergency room
ETT endotracheal tube
ICUintensive care unit
RUL right upper lobe
VQ ventilation-perfusion